Analysis: #COVID19 and tropical climate: can warm weather stop its spread in Africa?
Belete Ayele (@adbelete), Tinsae Alemayehu (@tinsaetigist) and Fitsum Tilahun (@fitse_t), For Addis Standard
COVID-19: A Once-In-A-Century Pandemic
Addis Abeba, March 23/2020 – A pandemic is a global outbreak of disease caused by a novel pathogen that spread between people because of little to no pre-existing herd immunity. Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first reported in Wuhan, Hubei Province, China on December 31, 2019 (Disease outbreak news; Jan 5, 2020, WHO). On March 11, 2020, WHO has formally declared COVID-19 a pandemic; the first coronavirus pandemic known to human. As of March 20, 2020, more than 270,000 confirmed COVID-19 cases from 164 countries are reported. Most research and guidance around respiratory virus pandemics are geared towards influenza pandemic mitigation; however, the same premises are being used to mitigate COVID-19 spread. Governments, philanthropists, public institutions, scientists, and the private sectors through global alliance are working day and night to quickly develop diagnostics, therapeutics, and vaccines and slow down the spread.
COVID-19 is a respiratory disease with efficient community transmission, primarily via respiratory droplets and fomites during close unprotected contact between humans. Household human-to-human transmission of COVID-19 occurs with as estimated secondary attack rate of 3-10% as per earlier report from China. Different countries are at different phases of the spread of COVID-19. Most COVID-19 cases (~80%) are mild; however, old age (age >65 years old) and comorbidities, such as hypertension, diabetes, chronic (lung, heart, kidney, and liver) conditions as well as immunocompromization have been identified as risk factors for severity and poor outcomes.
Not surprisingly, conspiracy theories, misinformation, and bad science are spreading as rampantly as the virus itself and it is our responsibility to teach the general public about the current state of the pandemic and provide effective precaution measures to mitigate the spread of COVID-19.
The Origin of SARS-CoV-2
SARS-CoV-2 is the third coronavirus after SARS-CoV and MERS-CoV known to infect and cause severe disease in humans. The other four human coronaviruses – HKU1, NL63, OC43, and 229E – cause only mild cold-like symptoms. To date, no animal coronavirus has been identified as the direct progenitor of SARS-CoV-2; however, a comparative genetic data analysis provided the strongest evidence for SARS-CoV-2 not to be a purposefully laboratory made virus (Andersen and colleagues, March 17, 2020, Nat Med). The genetic data irrefutably show that SARS-CoV-2 is not derived by reverse genetics from any previously known virus backbone. However, its exact origin is yet to be determined, and the authors proposed two plausible scenarios: (i) natural selection in an animal host before zoonotic transfer to human; and (ii) natural selection in humans following zoonotic transfer.
SARS-CoV-2 is ~96% identical at nucleotides level to the bat coronavirus, RaTG13; however, its receptor binding domain (RBD) in the spike protein is divergent, suggesting that RaTG13 may not efficiently bind to human ACE2 and hence it has to be adapted. Malayan pangolins, illegally imported into Guangdong province of China, contain SARS-CoV-2-like coronaviruses that have a profound similarity to SARS-CoV-2 in the RBD but are divergent in other regions of the genome. More sampling of the environment and sequencing is warranted as the diversity of coronaviruses in bats and other species is massively under sampled. To this end, the timing of the most recent common ancestor analysis for SARS-CoV-2 is compatible with the earliest retrospectively confirmed cases in Wuhan, China, which is around November to December 2019.
Learning from Past Epidemics
Transmission dynamics of any outbreak are inherently contextual; however, we can faithfully extrapolate from past epidemics growth phases and subsequent post-control periods. For instance, the 1918 influenza pandemic often referred to as the “Spanish Flu” killed an estimated 50 million people worldwide; the highest death rate was reported among healthy adults 15 to 35 years of age. The 100-year anniversary of the “Spanish flu” is a milestone, which unfortunately is marked by the emergence of a potentially rival COVID-19 pandemic. COVID-19 behaving a lot like a once-in-a-century pandemic and we should assume that it will be as bad as Spanish flu, if not worse. The world has also experienced three other flu pandemics in 1957 (H2N2 Flu), 1968 (H3N2 Flu), and 2009 (H1N1 Flu) as well as the two novel coronavirus epidemics in 2003 (SARS) and 2012 (MERS) in the past century, none of them were as severe as the Spanish flu.
Modern times epidemics are spreading faster and farther than ever because of the ease of intercontinental flights, which makes outbreaks containment an impossible undertaking (fig 1). A new disease can be introduced within hours from one to the other side of the world before even the affected individual knowns that he or she contracted the pathogen. For example, the 2009 influenza pandemic and the 2015 Korean MERS outbreak archetypal modern outbreaks that spread in a short space of time. COVID-19 has now garnered international attention and concern as a high severity pandemic; it spreads rapidly and efficiently between people and causes severe illnesses. Besides the virus-intrinsic virulence factors, the global aircrafts traffic, globalization, and mass gatherings facilitated COVID-19 worldwide spread affecting well over a quarter of a million people in less than three months. It has the potential to outpace the 1918 “Spanish flu” pandemic. Its ruinous impact on the global economy has already sent earthquake across different business, travel, trade, and basic livelihoods.
Fig 1: COVID-19 spread. Faster and farther with greater impact. Source: Managing Epidemics, WHO 2018
Calendar of Epidemics
Many infectious diseases are seasonal; seasonality varies by location (Martinez et al., PLoS Pathogens, 2018). Different diseases have different patterns depending on environmental factors, such as temperature, humidity, and latitude. Many others spread perennial. Surprisingly, COVID-19 combines efficient transmissibility with high fatality rate. The current models based on what we know predicts that SARS-CoV-2 could end up infecting ~65% of the world population; however, we do not know whether it will change its behavior in warm and humid weather, nor it could defy such pattern this year and subsequently, keeps spreading because of lack of enough herd immunity.
For example, Influenza spreads in winter in the norther hemisphere and difference in temperature, humidity, and human behavior are implicated for such seasonality. Although one could postulate about COVID-19 also being seasonal, we should assume that it will continue spreading in the next year until we know otherwise. Obviously, understanding its seasonality and the effect of climate will be informative to prioritize our investment in disease surveillance, timing of vaccination campaigns, and preparation for future epidemics.
Factors Influencing Seasonal Respiratory Virus Transmission
We do not know the exact mechanisms why many respiratory viruses (re-)emerge and hit humans like clockwork in in winter months the northern hemisphere; however, a multitude of factors – viral, human behavior, and environmental factors – were identified to modulate the calendar of viral epidemics.
- Viral factors
Viruses package their genetic material in a capsid protein. Some have an extra lipid bilayer membrane called envelope, which is essential to interact with the host cells during infection and to evade the host innate immunity. Low temperature and humidity modulate the properties of viral surface proteins and lipid membrane and hence increase viability of viruses that infect humans in temperate zone during winter (table 1). A recent study from the University of Edinburgh showed that enveloped viruses like RSV, influenza, and human metapneumovirus peak only in winter months whereas non-enveloped viruses, such as rhinoviruses and adenoviruses rather circulate in spring and summer months (Ramalingam and colleagues, Scientific Reports, 2018). Such seasonality was postulated to be due to a sharp drop in absolute humidity – the total amount of water vapor in a given volume of air. Indeed, Shaman and Lipsitch from Harvard observed a strong associated between the onset of new influenza epidemics and the start of cold and dry seasons (PLOS Biology, 2010). Coronaviruses, including SARS-CoV-2 are also enveloped viruses; the three common cold causing strains – HKU1, NL63, and OC43 – are seasonal, essentially behave like the flu (Kate Templeton and colleagues, J. Clinical microbiology, 2010). On the other hand, SARS-CoV that fizzled in the summer of 2003 and MERS-CoV, which continues to sporadically spread in humans did not circulate at larger scale for long enough period to determine their seasonality. The current pressing question is whether the COVID-19 outbreak will end in the spring and summer months? Although it is expected to be vulnerable to the increasing temperature and humidity of summer months and possibly be weakened or disappear. Currently, we do not know. Time will tell,
Knowing that SARS-CoV-2 spread between humans through droplet and fomite, understanding its viability outside human body is critically important. A recent study done in an optimized laboratory conditions determined the stability of SARS-CoV-2 and SARS-CoV and found that the two viruses behave the same (Munster and colleagues March 17, 2020, NEJM). They were able to retrieve viable viral particles in aerosol, on cardboard, on plastics and on stainless steel after 3, 24, 48, and 72 hours, respectively. Both SARS-CoVs exhibit comparable biophysical properties, therefore the major difference in the epidemiological characteristics of SARS-CoV compared to SARS-CoV-2 probably arose from the high viral loads in the upper respiratory tract and strong affinity to bind to its receptor, ACE2 of the latter.
Table: Effect of humidity on respiratory virus transmission in different climates and seasons
| Region/Season | Absolute outdoor humidity | Virus viability | Transmission mode |
| Tropical (Perennial) | High | High | Droplet, fomite, direct and indirect contact |
| Northern Hemisphere (Spring and summer) | Intermediate | Low | Droplet, fomite direct and indirect contact |
| Northern Hemisphere (Winter) | Low | High | Predominantly aerosol but also droplet, direct and indirect contact |
- Human Behavior
Human behavioral patterns affect the contact frequency and duration between transmitting and susceptible individuals. In cold weather, humans tend to spend more time indoors with less ventilation and less personal space than outdoors. For example, schools and other social gatherings are known to facilitate transmission of respiratory viruses, including chicken pox, measles, and flu. Moreover, easy and fast intercontinental travels are becoming major concern in spreading emerging epidemics faster and wider than ever. COVID-19 has become a global threat primarily because of intercontinental and across regional boundaries travels.
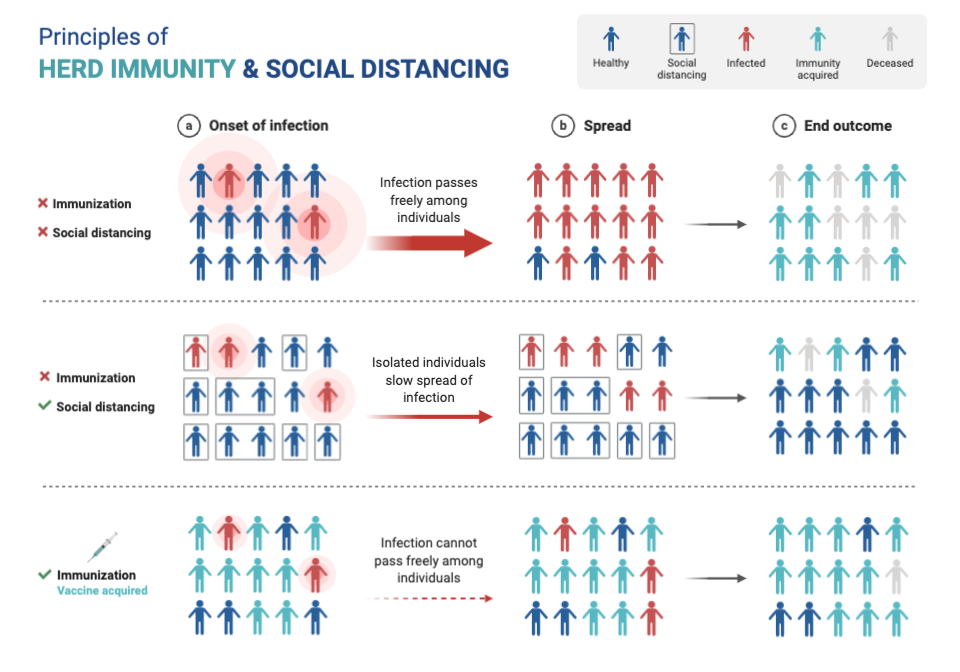
School closure was mandated worldwide in regions where community transmission was detected. Children are as susceptible and infectious as adults, but they do not develop severe COVID-19. The underlying factor(s) is yet to be identified. As human behavior continues to change, a significant epidemic response systems and strategies change is required to effectively and efficiently counter future epidemics. Meanwhile, social distancing by self-isolating and quarantine as well as practicing safe hygiene precautions remain the only effective measures to slowdown the spread of COVID-19 (fig 2).
- Influence of Climate and Seasons
“Respiratory diseases can spread efficiently in winter not necessarily because the temperature but because human beings come together in closed environments and therefore transmission is more facilitated. We have seen COVID-19 now in a number of different climates” Dr. Michael Ryan, WHO.
The above two factors i.e. viability respiratory viruses and host susceptibility have been experimentally shown to be affected by environmental factors. Absolute humidity change strongly affects flu transmission; cold and dry conditions favor flu spread. COVID-19 is a pandemic spreading to more than 160 countries of all climate zones. For instance, 1) a recent retrospective analysis (Luo et al., https://www.medrxiv.org/content/10.1101/2020.02.12.20022467v1) from 19 provinces (ranged from cold and dry to tropical climate) in China showed sustained COVID-19 spread in all provinces; 2) Singapore, one of the earliest countries to report COVID-19, lies near the equator and reported more than 250 COVID-19 cases of community spread; and 3) Several hundred COVID-19 cases were also reported in Africa. These examples strongly suggest that SARS-CoV-2 can sustain community transmission in all climate conditions of this time of the year.
Another modeling study concluded that sustained COVID-19 transmission appears to occur only in specific latitude bands with temperatures range of 5°C-11°C and relative humidity of 47%-70% (Sajadi et al, Preprint: http://dx.doi.org/10.2139/ssrn.3550308f) (Fig 3). The authors argued that most COVID-19 local transmission are from the northern hemisphere. Similarly, the 2003 SARS outbreak did not affect Africa or South America on a large scale, further supporting the notion that enveloped respiratory viruses tend to spread more effectively in winter months. In animal models, an ideal relative humidity for preventing aerosol respiratory virus transmission at room temperature (~22-24ᴼC) is between 40% and 60%. However, the lower temperature during the rainy season the tropical region may compensate for the high relative humidity (>60%) supporting severe COVID-19 spread.
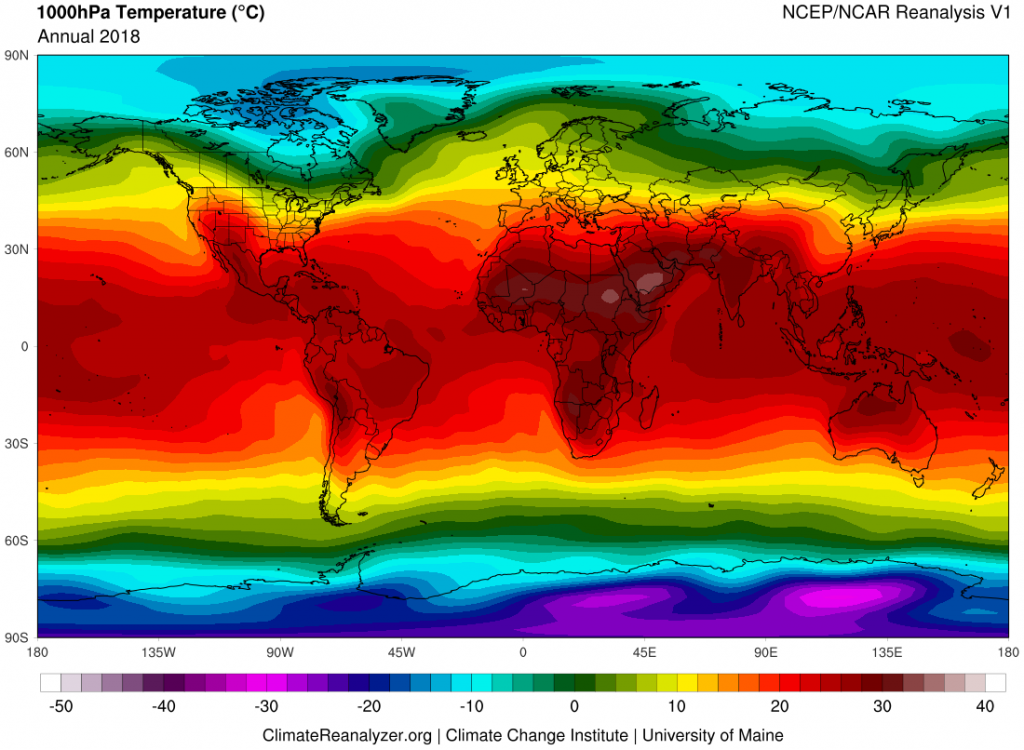
Fig 3. Average annual world temperature map for 2018. Tropical zone is delimited in latitude by the Tropic of Cancer in the Northern Hemisphere at 23.4N and the Tropic of Capricorn at 23.4S. Color gradient indicates 1000hpa Temperatures in ᴼC. Image from Climate Reanalyzer (https://ClimateReanalyzer.org), Climate Change Institute, University of Maine, USA.
FThe human airway mechanochemical defense can be affected by the seasonal clockwork in temperature and water content of the inhaled air. The respiratory tract mucus is a major barrier through its mechanical and biochemical antimicrobial properties. For instance, change in the chemical composition of mucus and subsequently impaired mucocilliary clearance under low temperature and low humidity predispose susceptible hosts to seasonal viral infection. Moreover, seasonal changes in daylight length, temperature and humidity in temperate zone shown to affetct the host antiviral immunity against respiratory virus infections. The innate “biological calendar” of the immune system believed to be associated with melatonin levels variation. Melatonin keeps track of the time of day but is also a “biological calendar” for the seasons; modulation of its secretion was shown to have an impact on the immune response (Hastings and Follett, J Biological Rhythms, 2001). Furthermore, genome wide analysis of samples taken from people in different parts (Europe, the United States, Gambia, and Australia) of the world revealed “seasonal expression profiles” for thousands of genes associated with immune function (Dopico et al., Nat Communications, 2014; Aguirre-Gamboa et al, Cell Reports, 2014). Therefore, the circadian rhythm of host immune system and seasonality of respiratory viral diseases are linked to environment factors.
In conclusion, not a single but a combination of climate-specific differences, including people living more outdoors than indoors, UV radiation, vitamin D levels, different daylight length, innate immunity, possible preexposure with coronaviruses, humidity, and temperature between northern hemisphere and tropical regions could slow down the spread of COVID-19 in Africa and other tropical regions (Hopman et al March 16, 2020 JAMA).
Conspiracy Theories and Myths
- SARS-CoV-2 is a laboratory engineered virus
Several conspiracy theorists continued their unfounded assertions by suggesting that SARS-CoV-2 is a purposefully laboratory engineered virus in China. Unfortunately, such misinformation has percolated into the general public and it is our duty to provide clarification and educate the public. To our relief, the elegant work that was just published in Nat Med by Dr. Andresen and colleagues irrefutably demonstrated that it is not a laboratory engineered virus. The genetic data analysis strongly indicates that SARS-CoV-2 was acquired via zoonotic transmission and through natural selection it has adapted to efficiently infect and spread in humans.
- COVID-19 will end on its own as the weather get warmer
The 2002 SARS did not die of natural course in summer months of 2003. It was eradicated by extremely intense public health interventions in China, the epicenter of the outbreak and other countries. Unlike COVID-19, the most infectious SARS cases were also quite ill in a distinctive way making isolation simple to contain it. Although COVID-19 is caused by a closely related coronavirus, it has strikingly distinct clinical and epidemiological characteristics. It spreads fast and efficiently between humans, including from mildly ill and asymptomatic cases.
COVID-19 spreads exponentially with a reproduction ratio (R0) of ~2-3 and prediction models, including one from CDC suggest that as much as 65% of the population could eventually be infected by SARS-CoV-2 if no action will be taken to slow its spread. The true course of the COVID-19 pandemic will, therefore, depend on better scientific information and the effects of the countermeasures, the current model suggest that the virus will spread widely over the next year.
Box: Tips to prevent respiratory virus transmission during epidemics
| Hand washing to prevent indirect contact transmission |
| Social distancing |
| Personal protective equipment only for health care workers and high-risk people |
| Wearing face mask if symptomatic and/or at high risk |
| Avoid nonessential travels and |
| Maintaining adequate indoor air ventilation and humidity |
| Vitamin D supplementation or adequate sunlight exposure |
| Maintaining optimal sleeping habit (sleep 7 -8 hours/day) |
- COVID-19 will not spread widely in Africa
The warm climate and living cultural differences in Africa have been postulated to be less amenable for efficient and rapid spread of COVID-19; however, COVID-19 spreading has already been confirmed in more than 30 countries in Africa. All identified index COVID-19 cases originated from Europe and not from China, even though there is a busy air travel traffic between China and Africa.
Most countries do not afford large-scale testing; thus, the true magnitude of the problem could be significantly underestimated. Another problem in Africa is the large-scale refugee camps and conflicts that can further fuel the COVID-19 spread and stress the limited health care facilities. Importantly, its impact on the already struggling economy will be unprecedented. Therefore, public awareness education and cost-effect pandemic response strategies should be implemented assuming that it will efficiently spread until we know otherwise.
- COVID-19 is just a “common cold” and only affects old people
Predicting how an emerging virus will behave based on past epidemics or closely related viruses that circulate in humans for long period is counterintuitive. For instance, we know that the epidemiological characteristics of SARS-CoV-2 are strikingly different from the other human coronaviruses and hence extrapolating the behavior of SARS-CoV-2 is a myth.
Another myth is that young adults develop mostly mild COVID-19 compared to the highly vulnerable elderlies and those with comorbidities. However, the latest reports from France, Italy, and USA indicate that it still can cause disproportionately higher rate of severe illness the young population than previously reported. Moreover, infectiousness remains high across the spectrum of the disease. Therefore, it is paramount to be vigilant in exercising the public health precaution measures and help to halt COVID-19 transmission.
In summary, SARS-CoV-2, like the other coronaviruses, transmits more efficiently in winter than summer months; however, supporting solid evidences are lacking. Epidemiological models suggest that SARS-CoV-2 could infect more than half the population of the world in a span of few months if left uncontrolled. Because of the speed and efficiency of COVID-19 spread and absence of robust herd immunity, the proportion of susceptible individuals expected to remain high, and thus expected to continue spreading in the next year. Social distancing and school closure could help to flatten the COVID-19 spread curve but are unlikely to completely stop its transmission. The role of asymptomatic and mildly ill adults and children in COVID-19 spread should be systematically addressed to implement effective prevention policies. The global COVID-19 pandemic responses brought more attention and prioritized investment in research and development. Scientists are working around the clock to develop innovative diagnostics, therapeutics, and vaccines by making significant systemic changes to alleviate the immediate crisis and respond more efficiently and effectively to future epidemics. AS